Comments
- No comments found

There's an old dream about preventive health care, which I still hear from time to time.
The hope is that by expanding the use of relatively cheap preventive care, then our society could either prevent some more extreme health conditions and/or catch and treat others early in a way that offers a double prize: it could conceivably improve both health and reduce total health care costs. But this happy outcome, while it may hold true in a few cases, is probably the wrong way to think about the economics of preventive medicine.
Joseph P. Newhouse addresses these questions in "An Ounce of Prevention" (Journal of Economic Perspectives, Spring 2021, 35:2, 101-18). By his estimate, only about 20% of preventive measures both improve health and save money. But when you think about it, most medical care doesn't save money: instead, it costs something for the benefit of improving health. In the same way, a wide array of preventive case can be worth doing because it improves health, even if it does not (on average) save money. Newhouse writes (citations omitted):
Vaccination is a well-known example of a measure that improves health and reduces cost. It is typically inexpensive, causes few adverse events, and can confer immunity for many years. The development of the polio vaccine, for example, was one of the great public health triumphs of the 20th century. In the late 1940s, polio crippled 35,000 Americans annually; because of vaccination, it was eradicated in the United States in 1979. Vaccination also differs from many other preventive measures because of the external benefit it confers on the unvaccinated (“herd immunity”). Another example of a preventive measure that saves money and improves health is a “polypill”—a single pill with several active ingredients for secondary prevention of heart disease versus single prescriptions for various agents.
The remaining 80 percent of preventive measures do not save money. The majority of all preventive measures—about 60 percent of them—provide health benefits at a cost of less than $100,000/QALY (2006 dollars). Another 10 percent of measures cost between $100,000 and $1,000,000 per QALY; those measures with costs near the lower end of this range might pass the common rules of thumb of cost-effectiveness ... The remaining 10 percent of preventive measures studied in the literature either worsen expected health or, if they improve it, cost more than $1,000,000 per QALY.
(For the uninitiated, "QALY" stands for "quality-adjusted life year," which is a way of measuring improvements in health. In this measure, a year in perfect health counts as 1, but gaining a year of impaired health counts less than one. For an overview, see "What's the Value of a QALY?")
Moreover, even if one focuses on a particular preventive measure, it will often be true that the potential health/income payoff for screening some people is higher than others. For example, if one group of people has a genetic predisposition or certain behavioral factors that make certain health conditions more likely, screening those is more likely to pay off with gains. It's quite possible to have situations where universal screening of all ages and groups may not be a cost-effective method of improving health, but screening higher-risk groups might make sense.
Newhouse also emphasized that it's useful to think about "preventive care" as meaning more than just medical interventions. For example, steps to reduce smoking and consumption of alcohol, or to encourage exercise, or to make sure that babies and small children have good nutrition, can have large payoffs.
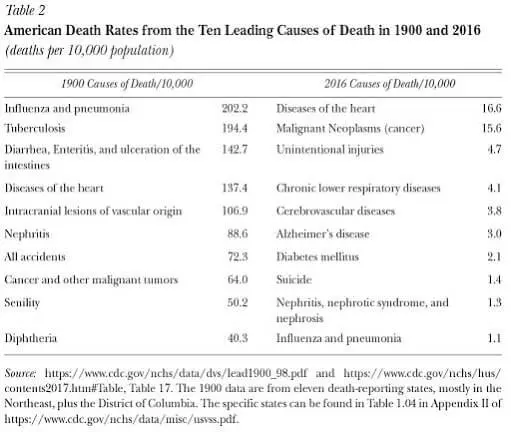
In addition, many of the steps used to address chronic health conditions are usefully thought of as "preventive case," like taking medications for high blood pressure. Indeed, one of the major shifts over the last century or so in US health patterns is that back in 1900, diseases were the major cause of death. Today after dramatic improvements in vaccinations and public health conditions, chronic diseases are the main causes of death. A "chronic" health condition can be loosely defined as one where if you take your meds, and follow the recommendations about what you consume, you can live pretty much a normal life, but otherwise, you have good chance of ending up with sharp decline in in health and a costly period of hospitalization. In the US, those with three more more chronic health conditions account for 61% of all health care spending. Thus, preventive measures to prevent chronic conditions from turning into something worse (both medical and non-medical) hold considerable promise in reducing health care costs. Here's a table from Newhouse:
Newhouse also discusses the incentive for innovators to develop methods of preventive care vs. developing new treatments. He argues that clinical trials are often much faster for treatment: for example, think about a firm trying to test whether a treatment extends the life of existing cancer patients vs. a firm trying to test whether a preventive treatments will reduce the long-run risk of a certain cancer occurring in the first place. In addition, a firm thinking about developing a preventive care approach must be concerned that many who are low-risk, or view themselves as low-risk, won't use the preventive care. However, if a firm develops a treatment for those who already have the health care condition, the chance of high demand for the product are much better.
A companion paper to the Newhouse essay in the same issue of the JEP looks at the controversial issue of mammograms. Amanda E. Kowalski writes: "Mammograms and Mortality: How Has the Evidence Evolved?" (Journal of Economic Perspectives, Spring 2021, 35:2, 119-40). There have been substantial controversies over the years on the recommended age at which women should start and stop getting regular mammograms. For example, prior to 2009, the US Preventive Services Task Force recommended regular mammographies for women 40 and over. However, the current guidance is regular mammographies for women 50-74, while leaving the decision up to women and their doctors for those outside that age range.
Why not just have universal mammograms for women of all ages? Sure, there's some cost, but "better safe than sorry" and "more knowledge can only be a good thing," right? As she points out, it's not that simple. Kowalski writes (citations omitted):
The rationale for widespread mammography is that early detection of potentially fatal breast cancers enables earlier and more effective treatment. But there is a potential drawback: mammography can detect some early-stage cancers that will never progress to cause symptoms—a phenomenon often referred to as overdiagnosis. In such cases, the emotional, financial, and physical costs of a cancer diagnosis and any subsequent treatments occur without any corresponding health benefit. Because it is hard to tell which women will be harmed by their cancers, there is a tendency to treat all women as if their cancers will be lethal. Even if the initial cancer would have never proven life-threatening, exposure to chemotherapy, radiotherapy, and surgery can potentially lead to new conditions, even to new fatal cancers ...
Just to be clear, "overdiagnosis" is not what is know as a false positive--that is, a screening which finds something that isn't there. Instead, "overdiagnosis" is finding something which is indeed there, but would not have caused a health problem. As she points out, a standard example is prostate cancer., and "autopsy studies showing that almost half of older men die with, but not necessarily of, prostate cancer have been important to prostate cancer screening guidelines since the late 1980s."
In practice, how big a problem is overdiagnosis from mammograms? There's some controversy over this evidence, but Kowalski makes a case that if the policy is to screen 100% of women in certain age ranges, the evidence (from randomized control trials done in Canada) is that over the long run, being randomly selected into the mammography group does not lead to an improvement in health on average--and may even be counterproductive. She writes that while most high-income countries still recommend regular mammography for asymptomatic women in their 50s and 60s, skepticism seems to be growing:.
Canadian national guidelines “recommend not screening” with mammography for women aged 40 to 49 but “recommend screening with mammography” for women aged 50 to 74. ... Many other high income countries, including Australia, France, Switzerland, and the United Kingdom, do not recommend mammography for women in their 40s, and they also do not recommend against it as Canadian guidelines do. However, the Swiss Medical Board recommended steps to limit screening programs in 2014. In 2016, the French Minister of Health released results of an independent review that recommended that the national screening program end or undergo radical reforms.
Her recommendations are for some additional research into understanding the characteristics--other than age--that are likely to make a mammography beneficial for women. In addition, when a mammography does find cancer, it may in some cases be wise to reduce or postpone the use of the most aggressive possible treatments.
Timothy Taylor is an American economist. He is managing editor of the Journal of Economic Perspectives, a quarterly academic journal produced at Macalester College and published by the American Economic Association. Taylor received his Bachelor of Arts degree from Haverford College and a master's degree in economics from Stanford University. At Stanford, he was winner of the award for excellent teaching in a large class (more than 30 students) given by the Associated Students of Stanford University. At Minnesota, he was named a Distinguished Lecturer by the Department of Economics and voted Teacher of the Year by the master's degree students at the Hubert H. Humphrey Institute of Public Affairs. Taylor has been a guest speaker for groups of teachers of high school economics, visiting diplomats from eastern Europe, talk-radio shows, and community groups. From 1989 to 1997, Professor Taylor wrote an economics opinion column for the San Jose Mercury-News. He has published multiple lectures on economics through The Teaching Company. With Rudolph Penner and Isabel Sawhill, he is co-author of Updating America's Social Contract (2000), whose first chapter provided an early radical centrist perspective, "An Agenda for the Radical Middle". Taylor is also the author of The Instant Economist: Everything You Need to Know About How the Economy Works, published by the Penguin Group in 2012. The fourth edition of Taylor's Principles of Economics textbook was published by Textbook Media in 2017.
BBN Times connects decision makers to you. Experts in their fields, worth listening to, are the ones who write our articles. We believe these are the real commentators of the future. We quickly and accurately deliver serious information around the world. BBN Times provides its readers human expertise to find trusted answers by providing a platform and a voice to anyone willing to know more about the latest trends. Stay tuned, the revolution has begun.
Leave your comments
Post comment as a guest