Comments (4)
Linda Davenport
Don't panic !!
Helen McKechnie
I miss 2019 so badly
Karl Reynolds
Holidays cancelled, work from home, no more school for kids, quarantine......
Danny Harris
Thanks for the info

No one will know for sure the best responses to the COVID-19 pandemic until after it's all over, and we look back and second guess ourselves.
Hindsight will approximate 20/20; foresight almost never does.
But as someone who has the same skin in the game as everyone else- my own, those I love- plus advanced training in epidemiology and public health- my view is that we are under-testing, over-reacting, and somewhat misdirecting our efforts.
Airborne infections with a fairly high rate of infectivity- and COVID-19 qualifies- simply spread too readily to cut off transmission without fully autocratic lock-downs, associated with martial law. It could theoretically be done, but the cost of doing it would likely exceed the cost of not- even in lives, as many of the most vulnerable would be most adversely affected by the disruption in goods and services. We would essentially need to hit the "pause" button on living, all but entirely.
There are exceptions, as ever, but the disease does not appear to affect children very severely (unlike the flu, which routinely kills young children). Healthy adults apparently mostly have a relatively mild illness and recover. The deaths among the elderly and ill tell us which population we should focus on protecting. I think we should be very carefully shielding our nursing homes and long-term care facilities; and we should be setting up free-standing (and, ideally, mobile) testing facilities away from hospitals and clinics- where, of course, older and sicker people tend to congregate.
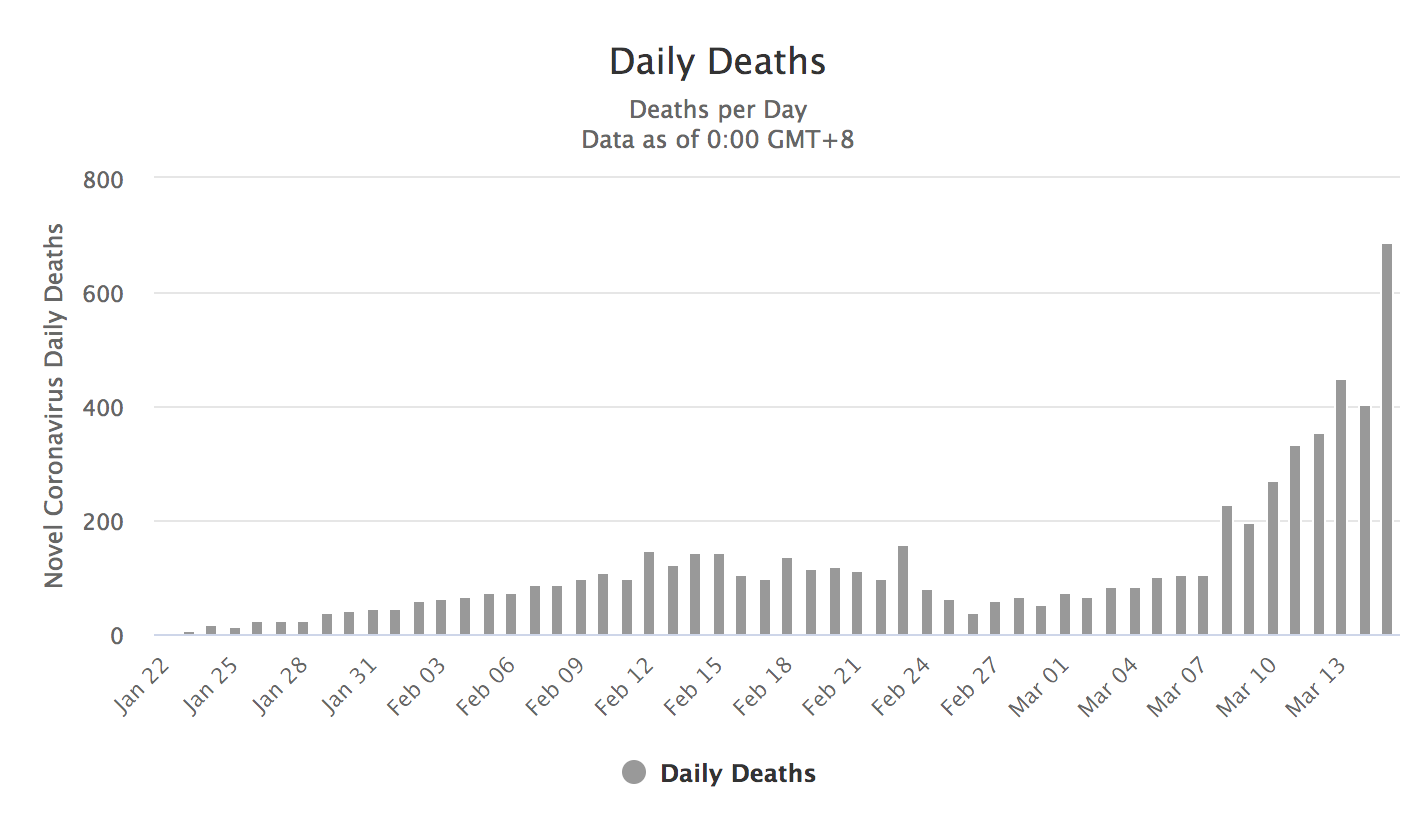
Importantly, the overall death rate is almost certainly much lower than the global figures suggest. Only in South Korea and on cruise ships has anything remotely like systematic testing taken place, and there- the mortality is slightly above 0.5% - nothing like the almost 4% reflected in the global data; nearly an order of magnitude less. This means death from the infection is much LESS likely than it seems, with the exception of the most highly vulnerable. But it also means that many, many more people around the globe are infected than we realize, because the numerator (i.e.g, deaths) implies the denominator (i.e., number infected). Italy, for instance, almost certainly has ten times as many cases as detected thus far. Most infected appear destined for fairly mild illness and recovery. But with so many already infected, spreading the virus without knowing it, infection for the rest of us is much MORE likely than the known cases suggest- meaning, this cat is already well out of the bag.
I am not convinced all of the burgeoning disruptions in the lives of children (i.e., school closings), young adults (i.e., changes in college and university routines), and working adults will prove of much value. People still need to shop for food, run critical errands, etc, and so- the virus will spread anyway. I think we are combining inconvenience and disruption with ineffective interdiction.
I, of course, am not in charge of any of this, but if I were- I would favor business as usual for the young and healthy; widespread testing AWAY from hospitals and clinics; enhanced home services for the frail, homebound elderly to shield them from outside exposure until this winds down; and "firewalls" of infectious disease interdiction around our nursing homes, care facilities, and hospitals. We are capable of this with a dedicated allocation of resources, and in my view, this "protect the most vulnerable, and carry on" approach would correspond most directly to the lessons to date in the global epidemiology of this disease.
At this point, a lot of us are going to get this virus almost no matter what we do, and the global data suggest that for most of us, it will be a fairly unremarkable respiratory illness followed by recovery.
Of note, the reaction to this pandemic is partly because it is genuinely serious, but partly because it is new, unfamiliar, and thus- not yet subject to our contempt. So far, as I write this, the global death toll from coronavirus is slightly under 7200. The death toll thus far this season from flu is nearly 100000. And, as noted, the flu is killing not just the elderly and sick, more prone to mortality from any cause, but children as well. Were the world tracking the "humble" flu with the same fixation directed to coronavirus, we would have at least 20X the basis for dread. And sure, there's a vaccine for flu- but there is also boisterous anti-vaccine nonsense all over the Internet, and many who should be defended against flu are not.
One thing for sure- we are all sharing an indelible moment in history. Only through the lens of history will we know exactly what we got right, and what we got wrong. Based on the view I have now, I fully expect that I, and/or someone I love, will get this infection- and I am confident it is unlikely to be too bad if we do. I am concerned, however, about my parents, mother-in-law, and other older relatives, and am conferring with family members about how best to protect them.
There are important lessons in this for preventing the next potential global pandemic; I certainly hope we learn them, although there, history is not all that encouraging. We seem much better at replicating the follies of history than learning from them.
And...we are, indeed, all in this together. That deserves more attention than it might command. This pathogen is telling us something we overlook far too readily: we are all more alike than different; all of a kind; vulnerable in the same general ways; all together on this one planet we all call home. There is no "us and them" to the coronavirus; we are all just us. It's a costly lesson, but at this divisive time- it is of great value.
Dr. David L. Katz is a board-certified specialist in Preventive Medicine/Public Health and...husband, father, son, brother.

Don't panic !!
I miss 2019 so badly
Holidays cancelled, work from home, no more school for kids, quarantine......
Thanks for the info
David L. Katz, MD, MPH, FACPM, FACP, FACLM, is the Founding Director (1998) of Yale University’s Yale-Griffin Prevention Research Center, and former President of the American College of Lifestyle Medicine. He has published roughly 200 scientific articles and textbook chapters, and 15 books to date, including multiple editions of leading textbooks in both preventive medicine, and nutrition. He has made important contributions in the areas of lifestyle interventions for health promotion; nutrient profiling; behavior modification; holistic care; and evidence-based medicine. David earned his BA degree from Dartmouth College (1984); his MD from the Albert Einstein College of Medicine (1988); and his MPH from the Yale University School of Public Health (1993). He completed sequential residency training in Internal Medicine, and Preventive Medicine/Public Health. He is a two-time diplomate of the American Board of Internal Medicine, and a board-certified specialist in Preventive Medicine/Public Health. He has received two Honorary Doctorates.
BBN Times connects decision makers to you. Experts in their fields, worth listening to, are the ones who write our articles. We believe these are the real commentators of the future. We quickly and accurately deliver serious information around the world. BBN Times provides its readers human expertise to find trusted answers by providing a platform and a voice to anyone willing to know more about the latest trends. Stay tuned, the revolution has begun.
Leave your comments
Post comment as a guest